

CASE 8
By: Dr. Saleh Othman, MD, MSc, JMCB
HISTORY: A 16-year-old male patient presented with fever, swollen painful right knee joint with limitation in movement and inability to walk. Bone scan requested because infectious process was highly suspected.
FINDINGS:
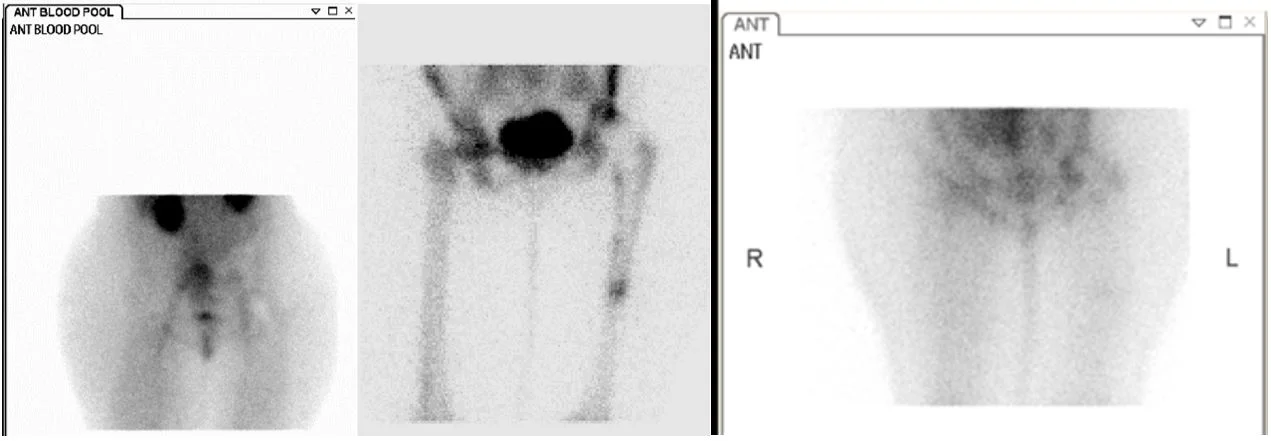
Three phase bone scan and gallium scan of both knee joints (anterior view).
Increased blood flow, blood pool and tracer uptake in bones of right knee joint on bone scan matched with increased gallium uptake of similar intensity. Findings are compatible with septic arthritis of right knee joint.
DIAGNOSIS:
Septic arthritis.

HISTORY: An 11-year-old boy with right ankle pain & persistent fever. Clinical diagnosis was osteomyelitis versus septic arthritis. Plain film was negative.
FINDINGS:
Three-phase bone scan and gallium scan of both ankle joints (anterior view).
Increased blood flow, blood pool and tracer uptake in distal end of right tibia (not crossing the joint) on bone scan matched with more intense gallium uptake. Findings are compatible with acute osteomyelitis of lower end of right tibia.
DIAGNOSIS:
Osteomyelitis.
PEARLS AND DISCUSSION:
Matched uptake of MDP on bone scan & gallium with same ore more intensity indicates active infection.
If gallium uptake is less then MDP, it indicates either chronic or partially treated infection.
When acute infection has been successfully treated, the gallium scan will usually return to normal while bony uptake of MDP remains high indication of repair process.
Bone scan (Blood pool) Bone scan (Delayed) Gallium scan
HISTORY: A 75-year-old female patient with left total hip replacement before 18 months. She presented with pain in left hip. Bone scan requested to evaluate the status of the prosthesis.
FINDINGS:
Bone and gallium scan.
Blood pool image: No hyperemia and photopenia in left hip region. Delayed image shows focal areas of increased uptake at femoral component of the prosthesis. Gallium scan unremarkable. Findings compatible with loosening with no evidence of active infection.
DIAGNOSIS:
Prosthesis loosening.
PEARLS AND DISCUSSION
Several complications can happen after joint prosthesis including loosening, infection, heterotopic bone formation, inflammatory bursitis and dislocation. Bone scan is helpful in differentiating loosening from infection. However, if complication is suspected radiograph is to be done first and if abnormal, manage accordingly but if its normal then three phase bone scan is to be done next completed with gallium or labeled white blood cell scan if infection is suspected.
Normal prosthesis will not show any increase in flow and pool images and delayed image will show photopenic area corresponding to the prosthesis.
Loose prosthesis will show normal flow, blood pool and focal areas of increased uptake at the tips of the femoral component.
Infected prosthesis will show diffuse increased flow, blood pool and tracer uptake around the prosthesis with matched increased gallium or WBC uptake.
Heterotopic bone formation will show increased uptake on delayed image outside the bone often parallel to the neck of the prosthesis.
Inflammatory bursitis will show focal increased flow, blood pool and tracer uptake in the bone which confine the prosthesis.
FURTHER READING:
Radiology 1985; Al-Sheikh W, et al. Subacute and chronic bone infections: Diagnosis using In-111, Ga-67 and Tc-99m MDP bone scintigraphy, and radiography. 155: 501-506
Ortho Clin N Am 1991; Wegener WA, Alavi A. Diagnostic imaging of musculoskeletal infection. Roentgenography; gallium, indium-labeled white blood cell, gammaglobulin, bone scintigraphy; and MRI. 22: 401-417
J Nucl Med 1998; Connolly LP, et al. Assessing the limping child with skeletal scintigraphy. 39: 1056-1061




